What to do if your over 100 days of Skilled Nursing Care?
Short answer: No — there is no rule that requires a skilled nursing facility (SNF) to charge the Medicare rate after day 100. After Medicare coverage ends, the facility can generally charge its normal private-pay rate, unless another payer (Medicaid/Medi-Cal, long-term-care insurance, etc.) applies.
What Medicare actually requires
Under Medicare Part A, SNF coverage is limited to 100 days per benefit period if the patient qualifies (e.g., after a 3-day inpatient hospital stay). (Aetna)
Cost structure:
-
Days 1–20: Medicare pays the full covered amount.
-
Days 21–100: Medicare pays most of the cost; the patient pays a daily coinsurance.
-
After day 100: Medicare stops paying entirely. (Solace)
Once that limit is reached:
“After 100 days, Medicare stops covering SNF care… you are fully responsible for all costs associated with continued care.” (Clara Home Care)
So the facility is not limited to the Medicare reimbursement rate after day 100; the resident becomes private pay unless another program covers the stay.
Why the “Medicare rate after 100 days” myth sometimes circulates
The confusion often comes from a few related rules:
-
Medicaid / Medi-Cal rules:
If a patient transitions to Medicaid (e.g., Medi-Cal long-term care), the facility must accept the Medicaid rate, which is usually much lower than private pay. -
Medicare-certified facilities:
While under Medicare coverage, they must accept the Medicare-approved payment as full payment for covered services. -
Medigap policies:
Some Medigap plans pay the daily coinsurance for days 21-100, which can make it appear that Medicare pricing continues longer.
But none of these require the SNF to keep charging the Medicare rate after day 100 if the patient stays privately.
Good primary citation
A clear government source is:
-
Medicare.gov — Skilled Nursing Facility Care
“Part A limits SNF coverage to 100 days in each benefit period.” (Medicare)
After those days, the beneficiary must pay the cost themselves.
✅ Bottom line:
-
Medicare pays up to 100 days of SNF care per benefit period.
-
After day 100, Medicare pays nothing, and the facility can generally charge its regular private-pay rate, not the Medicare rate.
If you’d like, Steve, I can also show you one obscure Medicare rule that sometimes helps people extend SNF coverage past 100 days indirectly (it’s a strategy used by elder-law attorneys and discharge planners).
The “60-Day Break” Rule (Benefit Period Reset)
Under Medicare Part A, the 100-day SNF limit applies per benefit period, not per year.
A benefit period ends when the patient has gone 60 consecutive days without:
-
inpatient hospital care, and
-
skilled nursing facility care.
Once that happens, a new benefit period begins, and the person can qualify for another 100 SNF days if the other conditions are met.
Citation
-
Centers for Medicare & Medicaid Services — Medicare & You handbook:
“A benefit period ends when you haven’t gotten any inpatient hospital care (or skilled care in a SNF) for 60 days in a row. If you go into a hospital or SNF after one benefit period has ended, a new benefit period begins.”
Source: Medicare & You 2026, Skilled Nursing Facility section.
How the “Reset” Strategy Works in Real Life
A typical scenario:
-
Patient receives 100 days of Medicare SNF care.
-
They are discharged to:
-
home,
-
assisted living, or
-
custodial nursing care (non-skilled).
-
-
60 days pass with no hospital or skilled SNF care.
-
Patient later has a new hospital admission (3-day inpatient stay).
-
They again qualify for up to 100 SNF days.
So theoretically someone could have multiple SNF benefit periods in one year if the timing works.
The Catch (Important)
To qualify again, the person must still meet all SNF requirements:
-
3-day inpatient hospital stay (observation days don’t count).
-
Need skilled care (rehab, IV therapy, wound care, etc.).
-
Admission to SNF within 30 days of hospital discharge.
Citation:
-
Centers for Medicare & Medicaid Services — Medicare SNF coverage rules (42 CFR §409.30).
Another Little-Known Rule
Sometimes facilities use the “skilled therapy requirement” interpretation:
If a patient still needs daily skilled therapy or nursing, Medicare may continue coverage within the 100 days even if improvement is slow or plateauing.
This came from the Jimmo v. Sebelius settlement, which clarified:
Medicare coverage does not require improvement, only the need for skilled care to maintain condition or prevent deterioration.
That ruling is extremely important in SNF appeals.
✅ Practical takeaway for your clients
For Medicare beneficiaries:
-
SNF coverage = up to 100 days per benefit period
-
Benefit period resets after 60 days without hospital/SNF care
-
A new hospital stay can trigger another 100-day cycle
If you want, I can also show you the nursing-home billing rule that actually does limit what they can charge in certain situations.
It’s obscure and very relevant to Medi-Cal / Medicaid patients in California, and it might have been what you originally heard about.
Steve, the rule you’re probably thinking about is the “bed-hold / leave day” and “no balance billing” framework for Medicare-certified nursing facilities. It doesn’t extend Medicare coverage, but it does restrict what facilities can charge in certain situations, which is why people sometimes think the facility must keep using the Medicare rate.
1. The “No Balance Billing” Rule While Medicare Is Paying
If a resident is in a Medicare-covered SNF stay, the facility must accept the Medicare payment plus any required coinsurance as full payment for covered services.
They cannot charge additional fees for services that are included in the SNF per-diem payment.
Citation
-
Centers for Medicare & Medicaid Services — Medicare Benefit Policy Manual, Ch. 8 §10
“The SNF must accept the Medicare payment as payment in full for covered services.”
This means a facility cannot bill extra “retail” charges for services included in the SNF benefit.
2. The “Leave Day / Bed-Hold” Rules
When a resident temporarily leaves a nursing facility (for example, hospital transfer or therapeutic leave), the facility sometimes cannot charge the resident privately for the bed during Medicare coverage.
These rules mostly arise from state Medicaid law and federal nursing-home regulations.
Citation:
-
Centers for Medicare & Medicaid Services — Nursing Facility Requirements
42 CFR §483.15
Facilities must clearly disclose bed-hold policies and cannot impose charges inconsistent with Medicare or Medicaid payment rules.
3. The Rule That Actually Limits Charges (Medicaid)
The strongest restriction is actually the Medicaid payment-in-full rule:
-
If the resident is Medicaid-eligible,
-
and the facility participates in Medicaid,
the facility must accept the Medicaid rate as full payment and cannot bill the resident extra.
Citation:
-
Centers for Medicare & Medicaid Services — 42 CFR §483.15(e)
“The facility must accept the Medicaid payment as payment in full.”
Why the Confusion Happens
Families often see something like this timeline:
-
Hospital stay
-
Medicare SNF coverage (up to 100 days)
-
Patient becomes Medicaid eligible
-
Facility switches from private pay rate ($10k–$15k/month) to Medicaid rate ($6k–$9k/month)
So it appears as though “the nursing home had to charge the Medicare rate after day 100.”
But in reality the change happened because Medicaid eligibility started.
Bottom Line
-
Medicare SNF coverage: 100 days max per benefit period
-
After day 100: facility may charge its private-pay rate
-
If Medicaid starts: facility must accept the Medicaid rate as full payment
💡 One last thing, Steve — because you work with Medicare clients, there is actually a frequently misunderstood SNF billing protection that can matter for beneficiaries with Medigap policies.
It relates to who is responsible if Medicare later denies a SNF claim after the patient was already admitted. The rule can prevent the patient from being billed thousands of dollars. If you want, I can show you that one too.
Long Term Care would work… if you do it prior to getting ill…


#Contact Us - Ask Questions - Get More Information - Schedule a Zoom Meeting
By submitting the information below , you are agreeing to be contacted by Steve Shorr a Licensed Sales Agent by email, texting or Zoom to discuss Medicare or other Insurance Plans as relevant to your inquiry. This is a solicitation for Insurance
Steve, the rule you may have heard about usually comes from Medicaid (Medi-Cal in California) nursing-home rules, not Medicare itself. There is a situation where a nursing facility cannot charge its retail/private-pay rate and must accept the government payment rate.
The “Medicaid Rate Must Be Accepted” Rule
Once a resident becomes eligible for Medicaid (in California, Medi-Cal long-term-care):
-
The nursing facility must accept the Medicaid payment rate as payment in full.
-
They cannot bill the resident extra beyond the required patient share of income.
Citation:
-
Centers for Medicare & Medicaid Services — Nursing Facility Services Regulations
“The facility must accept, as payment in full, the amounts paid by Medicaid… and may not charge the resident additional amounts.”
— 42 CFR §483.15(e)
This is often called the “no balance billing” rule.
What the Resident Still Pays
The resident usually must pay a patient liability amount, which is basically:
Monthly income
– personal needs allowance
– certain deductions (spouse allowance, health insurance premiums, etc.)
Whatever remains is paid to the facility, and Medicaid pays the rest.
In California this is often called the “share of cost” for long-term care.
Why People Confuse This With Medicare
A typical timeline looks like this:
-
Hospital stay (3+ inpatient days).
-
Medicare SNF coverage
-
Days 1–20: Medicare pays fully
-
Days 21–100: patient coinsurance
-
-
After day 100:
-
Patient becomes private pay unless they qualify for Medicaid.
-
-
If they qualify for Medicaid long-term care, the facility must accept the Medicaid rate, not the private-pay rate.
So sometimes families see the bill drop dramatically and assume there was a “Medicare rate limit after 100 days.”
But the real reason is Medicaid eligibility kicked in.
Important California Rule
Under California Medi-Cal law, a nursing home that accepts Medi-Cal generally cannot require a resident to remain private pay for a certain period before converting to Medi-Cal.
Citation:
-
California Department of Health Care Services — Medi-Cal Nursing Facility Provider Manual.
Facilities cannot refuse to accept Medi-Cal payment for an eligible resident if they participate in the program.
✅ Bottom line
| Situation | What the facility can charge |
|---|---|
| Medicare SNF days 1–100 | Medicare-approved rate |
| After day 100 (private pay) | Facility’s normal retail rate |
| After Medicaid/Medi-Cal eligibility | Must accept Medicaid rate as full payment |
If you’d like, I can also show you another extremely obscure Medicare SNF rule that elder-law attorneys use — it allows Medicare to continue paying beyond 100 days in rare situations due to technical discharge/readmission timing rules. It’s buried in the Medicare Benefit Policy Manual and hardly anyone knows it.
Steve, there is a very obscure Medicare SNF rule that can sometimes allow coverage to go beyond what people think is the 100-day limit, but it doesn’t actually extend the limit — it creates a new 100-day benefit period through timing and discharge rules.
This comes from the Medicare Benefit Policy Manual.
The “Benefit Period Reset Through Custodial Care” Strategy
If a patient stops receiving skilled care but remains in the nursing facility for custodial care only, Medicare coverage stops — but the benefit period may still continue running.
However, if the patient later leaves skilled care long enough to end the benefit period, a new benefit period can start, creating another 100 days of SNF coverage.
Key rule
A benefit period ends when the patient has gone 60 consecutive days without:
-
inpatient hospital care, and
-
skilled nursing facility care.
Citation:
-
Centers for Medicare & Medicaid Services — Medicare Benefit Policy Manual, Ch. 8 §10
“A benefit period ends when the beneficiary has not received inpatient hospital care or skilled care in a SNF for 60 consecutive days.”
Once that happens, a new benefit period begins, allowing:
-
20 fully covered SNF days
-
80 coinsurance SNF days
for another 100-day cycle.
The Rare “Technical Discharge / Readmission” Situation
Sometimes facilities structure discharges like this:
-
Patient uses most or all of the 100 SNF days.
-
Patient leaves skilled care (home, assisted living, custodial nursing).
-
60 days pass with no skilled care.
-
Patient has a new qualifying hospital admission.
-
Medicare SNF coverage starts again with a fresh 100 days.
This can happen multiple times in a year if the timing works.
The Rule Most People Don’t Know (Jimmo Settlement)
Another major misunderstanding used to shorten SNF coverage was the belief that a patient must be improving.
That changed after:
-
Jimmo v. Sebelius
The settlement clarified:
Medicare coverage does not require improvement, only the need for skilled care to maintain or prevent deterioration.
This is why some patients successfully appeal SNF terminations and continue coverage within the 100-day period.
Citation:
-
Centers for Medicare & Medicaid Services — Jimmo Settlement Fact Sheet.
Why This Matters for Your Clients
Many Medicare beneficiaries are discharged before day 100 because facilities claim they are not improving.
But under Jimmo, Medicare must continue paying if:
-
skilled therapy is required to maintain function, or
-
skilled nursing is required to prevent deterioration.
This is one of the most common successful Medicare appeals in skilled nursing cases.
✅ Simple takeaway
| Rule | What it means |
|---|---|
| SNF coverage | Up to 100 days per benefit period |
| Benefit period reset | 60 days with no hospital or skilled care |
| New hospital stay | Can trigger another 100 SNF days |
| Jimmo rule | Improvement not required for coverage |
💡 Since you deal with Medicare a lot in your insurance work, there’s actually one even stranger rule that affects SNF billing and could have been the one you originally read about — it involves “bed-hold” and “leave days” where facilities sometimes must bill at Medicare rates even when Medicare isn’t paying.
If you want, I can show you that one too — it’s buried in 42 CFR nursing facility regulations and very few brokers know it.
See our webpage on balance billing & no surprises act
How does Medicare pay for #SkilledNursing Homes - 10153 11359
Our Introductory You Tube VIDEO based on this manual

- Your costs for Skilled Nursing in Original Medicare You pay:
-
Days 1–20: $0 for each benefit period .
- Days 21–100: $194.50 coinsurance per day of each benefit period.
-
Days 101 and beyond: All costs. Medicare.gov *
-
- Clinical Guidelines explain the coverage so much better and in logical order!
- The two-midnight rule and Medicare Advantage: 7 updates Beckers Payer.com 2/2024
- Medi Cal Payments Fall Far Short of Covering Care Costs at Nursing Homes Skilled Nursing News.com 11/2024
- Medicare's VIDEO Nursing Home / Long-Term Care
- Planning for Discharge from a Health Care Setting VIDEO
- Long Term #Acute Care Publication # 11347
- Differences between Skilled Nursing, Long Term Acute Care & Inpatient Rehabilitation Facility
- Our FAQ on Sub Acute Care
- Find & compare nursing homes, hospitals & other providers near you Medicare.Gov
- Learn more about providers
- Calculate Cost of Long Term Care in your Area Genworth
- "Hospital at Home" Programs Improve Outcomes, Lower Costs But Face Resistance from Providers and Payers
- Pro Seniors Medicare & Skilled Nursing
- Medicare doesn't pay for:
- Our Webpagse on Long Term Care
See our page on acute care…
#My Medi-Cal
How to get the Health Care
You Need
24 pages
Smart Phones - try turning sideways to view pdf better


-
Brother – Sister – Sibling Side Pages Subpages

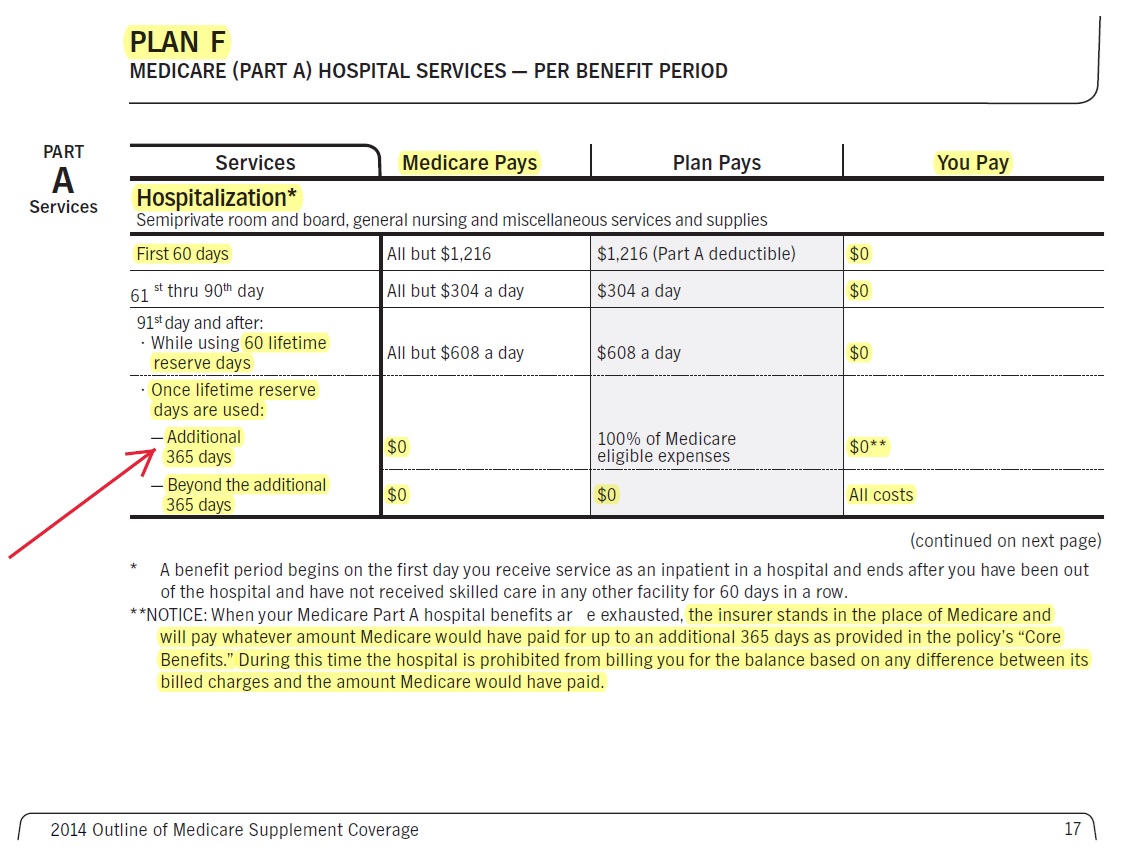
How does Medi Gap Plan Hi F pay for Hospital Care, Long Term #Acute Hospital, Sub Acute Care, Skilled Nursing, Home Health Care?
What happens if you go over 90 days? How do 60 lifetime reserve days work? How do 365 additional from Medi Gap work?
Email us [email protected] for Source Brochure

[Hi Steve]
The case manager looked into my mom’s secondary insurance [redacted] and they are going to cover 30 days in the long term acute care facility, which is huge.
This is really stressful, and I truly appreciate you taking your time during your time with your family. I’m not Jewish, but I recognize a Mitzvah when I see one.
Mike
In common parlance, a mitzvah often refers to a “good deed” or act of kindness.
https://www.chabad.org/library/article_cdo/aid/1438516/jewish/Mitzvah.htm